



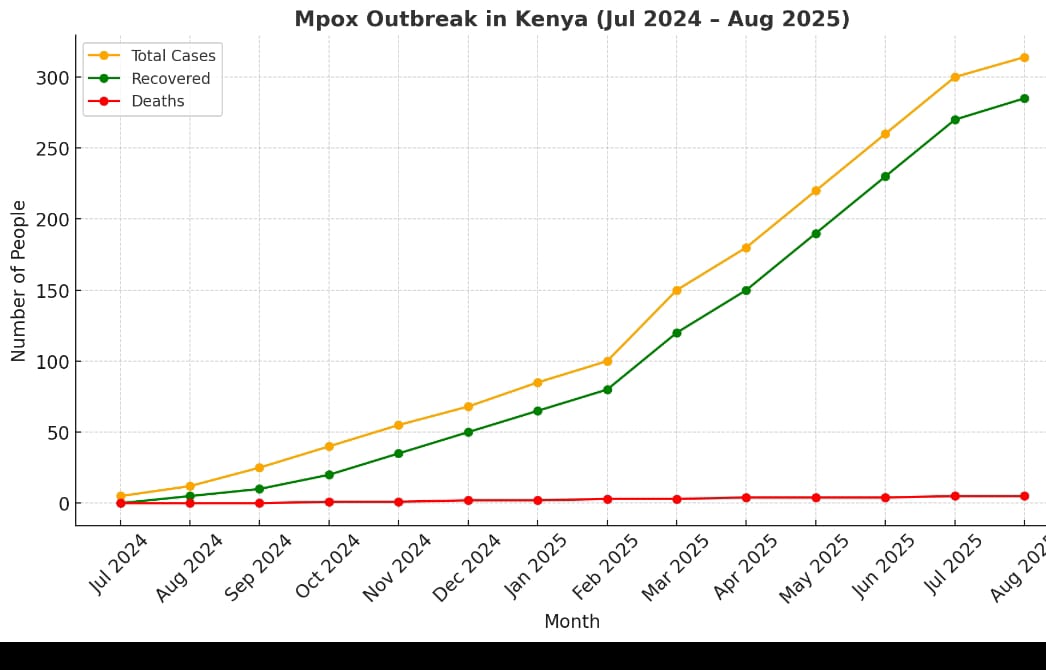
Kenya is confronting an alarming mpox outbreak that doesn’t just knock at the door—it’s barged right in. Since the first confirmed case at the Taita-Taveta border point on July 31, 2024, a wave of infections has swept across 22 counties, pushing total cases to 314 as of early August 2025—and with five tragic deaths recorded so far.
What began as a few sporadic infections has evolved into a tide. In just the past three months, cases have nearly quadrupled—from 68 in April 2025 to 314 by late July—no small uptick in a country still finding its public health rhythm. The virus’s reach spreads unevenly but ominously—Mombasa remains the epicenter with 146 cases, trailed by Busia with 63, then Nakuru, Kilifi, Nairobi, and others in descending order.
Mpox, caused by the clade Ib variant—a more transmissible and potentially severe strain—began this chapter in Central Africa before crossing borders. Now it’s here.


Symptoms aren’t subtle. They begin with fever, headache, swollen lymph nodes, and intense muscle aches. Days later, the hallmark rash erupts—pustules that scab, fall off, and leave scars. The discomfort? Harrowing—and that’s just the beginning.
While most patients recover fully in 2 to 4 weeks with supportive care—rest, hydration, fever relief, and clean wound care to avert secondary infections—this isn’t universally true. The fatality rate across the broader clade Ib outbreak in Africa hovers at ~3%, especially where medical infrastructure is strained. In Kenya, though lower so far, every death is a signal that mpox cannot be shrugged off.
Read Also: Don’t Deny Smokers Their Best Chance Of Dodging Diseases
Treatment remains a mixed picture. There’s no mpox-specific approved therapy, but tecovirimat (TPOXX)—an antiviral originally developed for smallpox—is available under compassionate use protocols for severe cases. However, clinical trials show tecovirimat is safe but doesn’t significantly speed up lesion healing in humans. In the Democratic Republic of the Congo, its benefits were largely limited to the sickest patients, while the majority saw no major improvements over placebo.

Still, there is a silver lining—and a reminder. Studies show that high-quality supportive care in a hospital setting dramatically lowers mortality, even when antivirals fall short.
The message is clear: this is not a disease to be ignored. Kenya’s mpox outbreak demands heightened alertness from every one of us. Health workers must intensify surveillance, contact tracing, and case isolation. Communities must recognize symptoms early, seek care promptly, and adhere to preventive measures—especially in hotspots like Mombasa. Public awareness campaigns should underscore how the virus spreads through close or skin-to-skin contact, contaminated items, or respiratory droplets.
The virus is here. It’s transmissible. It can kill. Without vigilance, its toll will grow. Let this report be the wake-up call: Kenya must stay alert—not just for itself, but for every community connected by proximity or travel.
Read Also: Non-Communicable Diseases Account For 27% Of Deaths In Kenya